tumor lysis syndrome
- related: Hemeonc
- tags: #hemeonc
Tumor lysis syndrome (TLS) occurs when a large tumor burden undergoes rapid destruction with release of its intracellular contents into the bloodstream. Resulting electrolyte and metabolic abnormalities can cause acute kidney injury (eg, calcium-phosphate precipitation in renal tubules), arrhythmias (eg, calcium-phosphate precipitation in the heart), seizures, and possible sudden cardiac death. TLS is defined by >2 of the following:
- Uric acid >8.0 mg/dL (or 25% ↑ in baseline value [BV])
- Potassium >6.0 mEq/L (or 25% ↑ in BV)
- Phosphorus >4.5 mg/dL (or 25% ↑ in BV)
- Calcium <7.0 mg/dL (or 25% ↓ in BV)
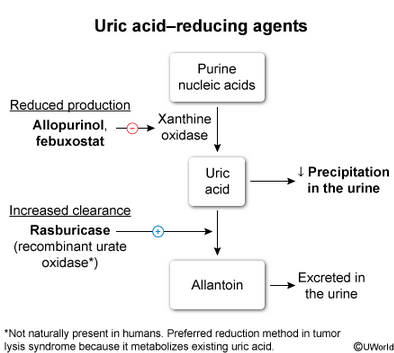
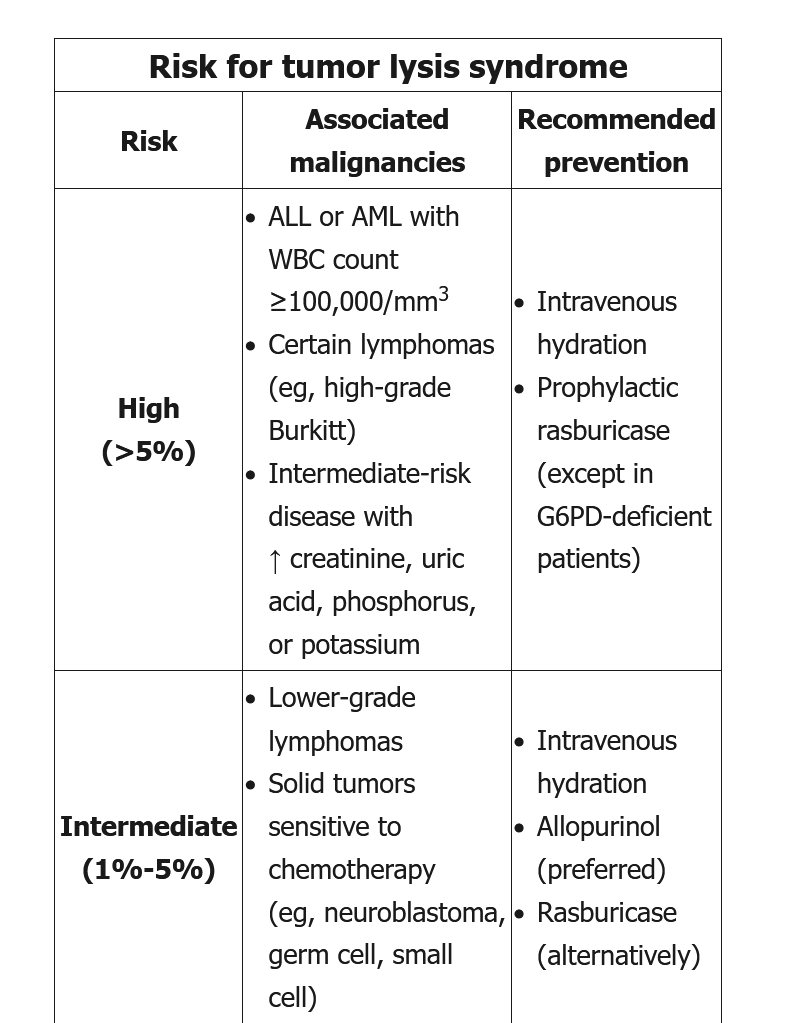
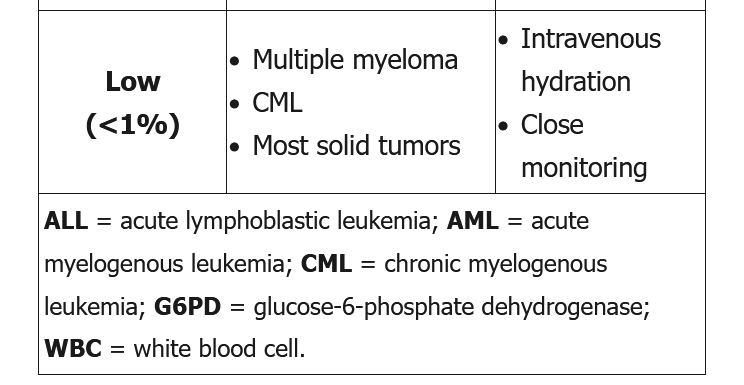
Strategies for TLS prevention are dependent on risk stratification (Table). Low-risk patients need only hydration with close monitoring, whereas intermediate-risk patients may receive hydration and allopurinol. High-risk patients should receive intravenous hydration and 5-7 days of prophylactic rasburicase, a recombinant uric acid oxidase that immediately catalyzes uric acid conversion into water-soluble allantoin and rapidly lowers uric acid levels.
Although this high-risk patient (with acute myeloblastic leukemia with leukocytosis >100,000/mm3) received appropriate prophylactic therapy, she has elevated phosphorus and potassium as well as worsening renal function, concerning for impending TLS development. She should receive aggressive intravenous hydration with a urine output goal of >80-100 mL/hr as this helps decrease formation of uric acid and calcium-phosphate crystals.
Allopurinol inhibits xanthine oxidase to prevent formation of uric acid and requires 3-4 days to become fully effective; it does not lower the preexisting uric acid levels. Regardless, this patient's uric acid level has already decreased, indicating that rasburicase was effective and should be continued.
Treatment includes aggressive IV fluids (with or without a loop diuretic) and urgent hemodialysis in severe cases. Commonly accepted indications for initiating short-term hemodialysis in patients with TLS include the following:
- Calcium phosphate product ≥70 mg2/dL****2 (87 in this patient)
- Symptomatic hypocalcemia
- Persistent hyperkalemia
- Severe oliguria or anuria
Early initiation of hemodialysis portends an excellent prognosis for renal recovery.
TLS
- LDH high: inside malignant cells, aerobic glycolysis
- ppx: allopurinol
- treatment: rasburicase